
Major health organizations have begun to recognize obesity as a disease. Ten years or earlier And the treatments range from behavior change counseling to bariatric surgery.A class of prescription drugs that could lead to significant weight loss (GLP-1) has emerged as a potential breakthrough treatment for the one-third of obese U.S. adults* (BMI must be 30 or above). However, health care coverage and access in the fragmented U.S. health care system is determined by many parties, with obesity rates in the state of residence providing coverage and thus how accessible this class of drugs is for patients. It can affect whether it is easy and affordable.
Looking at the KFF’s State Health Facts index, which shows the distribution of adults with a body mass index (BMI) of 30 or higher, the 20 states with the highest obesity rates are all in the Midwest and South. Classified According to the U.S. Census Bureau (Figure 1).
Comparing mean obesity rates by region (Figure 2), adult rates in the Midwest and South are about 5 percentage points higher than in the Northeast and 6 percentage points higher than in the West.
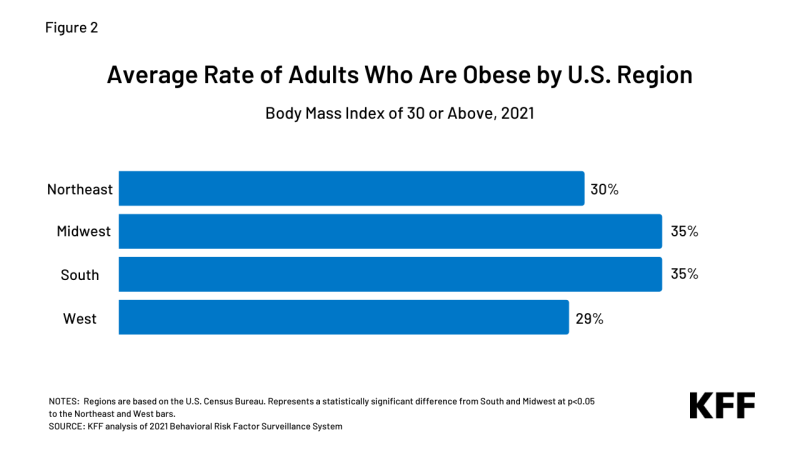
Figure 2: Mean age of obese adults by US region
The cost of treating obese adults with GLP-1 drugs is high in the short term and may affect insurance coverage policies. Medicaid programs in Midwestern and Southern states, as well as employers and insurance companies with a large presence in these regions, may factor high rates of obesity in their populations into their decision making. In addition, 7 out of 10 states have not adopted Medicaid expansion as a factor in access to these medicines, and nearly all of them experience coverage gaps because it is not expanded. (97%) live in the South.
Currently, Medicaid coverage for drugs prescribed for weight loss varies by state, but is generally limited for GLP-1 drugs, and employer-based and private insurance coverage for weight loss drugs also varies. Masu. The Medicare program does not cover weight-loss drugs because they are prohibited by law.
Recent reports (business insider, status, WSJMore) Some employers previously covered by GLP-1 drugs have withdrawn their coverage, revealing that health insurance companies are scrutinizing doctors’ off-label prescriptions. Continued FDA approval of this type of drug is expected to significantly increase costs, and coverage for the drug could stagnate, shrink, or be limited, including by limiting eligibility for those with a high BMI. be. (Obesity is generally categorized as follows) three ranges of BMI. The American Medical Association recently Clarified policy on the role of BMI as a measure of obesity, discusses historical issues and their limitations. ) Other possible actions include:
- Limit off-label use,
- If you need additional treatment, such as behavioral therapy in combination with drugs,
- Pre-approval, including step therapy to try cheaper options first, and
- Higher cost sharing.
Early clinical results and the potential for new prescription drugs for weight loss are of interest to nearly half of US adults. Federal and state policymakers, employers, and insurance coverage companies should consider the potential costs and benefits of these drugs when deciding whether and how to cover them in insurance plans. It’s in early stages. The long-term cost savings from reducing obesity and its associated risks in the country could be substantial. nevertheless, Current prices in the United States for these weight loss drugs are high And lifelong use may be required for continued health benefits. Among the patients prescribed the drug, experiencing side effects And the long-term effects of its use remain questionable.
Adult obesity rates are high in the Midwest and South, and state health systems and local employers may face rising health care costs, especially in the short term, and seek ways to control the use of new weight-loss drugs. have a nature. Regional trends may differ as the coverage of GLP-1 prescription drugs increases.
*U.S. Centers for Disease Control and Prevention (CDC) National Health and Nutrition Examination Survey estimates that approximately 4 in 10 adults are obese using clinical measurements. KFF estimates are based on state-level behavioral risk factor monitoring analysis. System self-reported data collected via phone call by CDC and state health departments.